After discussion with like-minded folks and research through the net, our Definition of an NGO needs a broader framework than what is usually understood.
Our Beneficiaries
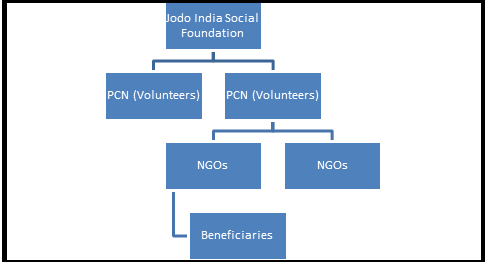
It is necessary to define our beneficiaries so that we may understand our needs of an ‘NGO’. Our chain of communication is as under:
Our Beneficiaries are Needy School-going girls in the age bracket of 8-16 years – so we may reach them just at the start of puberty/menstruation cycles. Our hope is that if we reach them first with reusable sanitary pads they are less likely to move to the use and throw variety.
Our target beneficiaries reside in villages or small towns (away from cities) that have government schools that are usually run by Zilla Parishads, i.e. government aided/run schools. It is here that we may find our needy beneficiaries.
This last-mile connection is among our bigger challenges. We would like to use the term NGO in a very broad manner: Any outfit/group that is
- Already doing work with such schools
- Has access to such school and beneficiaries
- Is willing to connect with our target beneficiaries
- Has a lady dominant partner/leader
So yes, we need to broaden our definition of a typical NGO. It is likely that typical (meaning registered) NGOs such as trusts and societies may also fall within our target NGO group. However, the ‘NGOs’ that we would look for are less likely to be located in cities and towns. They may be located in larger towns and even cities, but either the NGO or one of their divisions/representatives/associates must be located near and focussed on villages.
NGOs that are either Trusts, Societies or Section 8 (formerly Section 25) companies must be validated in accordance with our guidelines given elsewhere.
Other ‘NGOs’ could be any of the following:
- SHGs (Self-Help Groups)
- Accredited Social Health Activist (ASHA). These are one of the key components of the National Rural Health Mission which is to provide every village in the country with a trained female community health activist ASHA. Selected from the village itself and accountable to it, the ASHA will be trained to work as an interface between the community and the public health system. Following are the key components of ASHA:
- ASHA must primarily be a woman resident of the village married/ widowed/ divorced, preferably in the age group of 25 to 45 years.
- She should be a literate woman with due preference in selection to those who are qualified up to 10 standard wherever they are interested and available in good numbers. This may be relaxed only if no suitable person with this qualification is available.
More information about this initiative is available on this site: http://nhm.gov.in/communitisation/asha/about-asha.html
- Individuals that are socially active and are either already dedicated to the cause or are willing to help us establish the last mile connectivity. These may be found through the net, through their blogs or their FB presence.